Optimizing the Aesthetic Outcome: The Vertical Position of the Maxillary Incisor
Serge Ketoff · Jean-Pascal Dujoncquoy · Mehdi Sersab · Alexia Gelas
CLINIC No. 452/453 · July–August 2025
The maxillary central incisor is a key element of the lower third of the face: it supports the upper lip and defines tooth display at rest and when smiling, as well as the amount of gingiva visible at maximum smile. Beyond the smile, its position determines mandibular position through occlusion. The orthodontic-surgical team must therefore decide: should this position be changed? If so, orthodontically, surgically, or both?
Facial Analysis: Three Key Parameters
First, facial height: when balanced, it allows lip contact at rest without contraction of the chin muscles, the face dividing into three equal thirds. Next, the lip position at rest: it should reveal approximately 2 mm of incisor in men and 4 mm in women — that is, one third of the incisor height. Finally, tooth and gingival display when smiling: a harmonious smile exposes 1 to 4 mm of gingiva. When rest and smile findings conflict, the rest position takes precedence for planning; the photographic record is ideally supplemented by a video recording of smile dynamics.
Case 1: Long Face (Facial Hyperdivergence)
The patient presents with a long face, lip incompetence, a gummy smile and excessive tooth display at rest. The surgical objective is to reduce facial height with an anterior impaction Le Fort I osteotomy combined with counterclockwise rotation of the occlusal plane, associated with mandibular advancement. This rotation projects the chin point and makes genioplasty unnecessary. The impaction must not be overestimated: upper lip lengthening with age, crown wear and the contribution of the anterior maxilla to nasal morphology must all be factored into the quantification. In women, a gummy smile is preferably undercorrected, otherwise an oval face risks being "squared off".

Case 2: Short Face (Facial Hypodivergence)
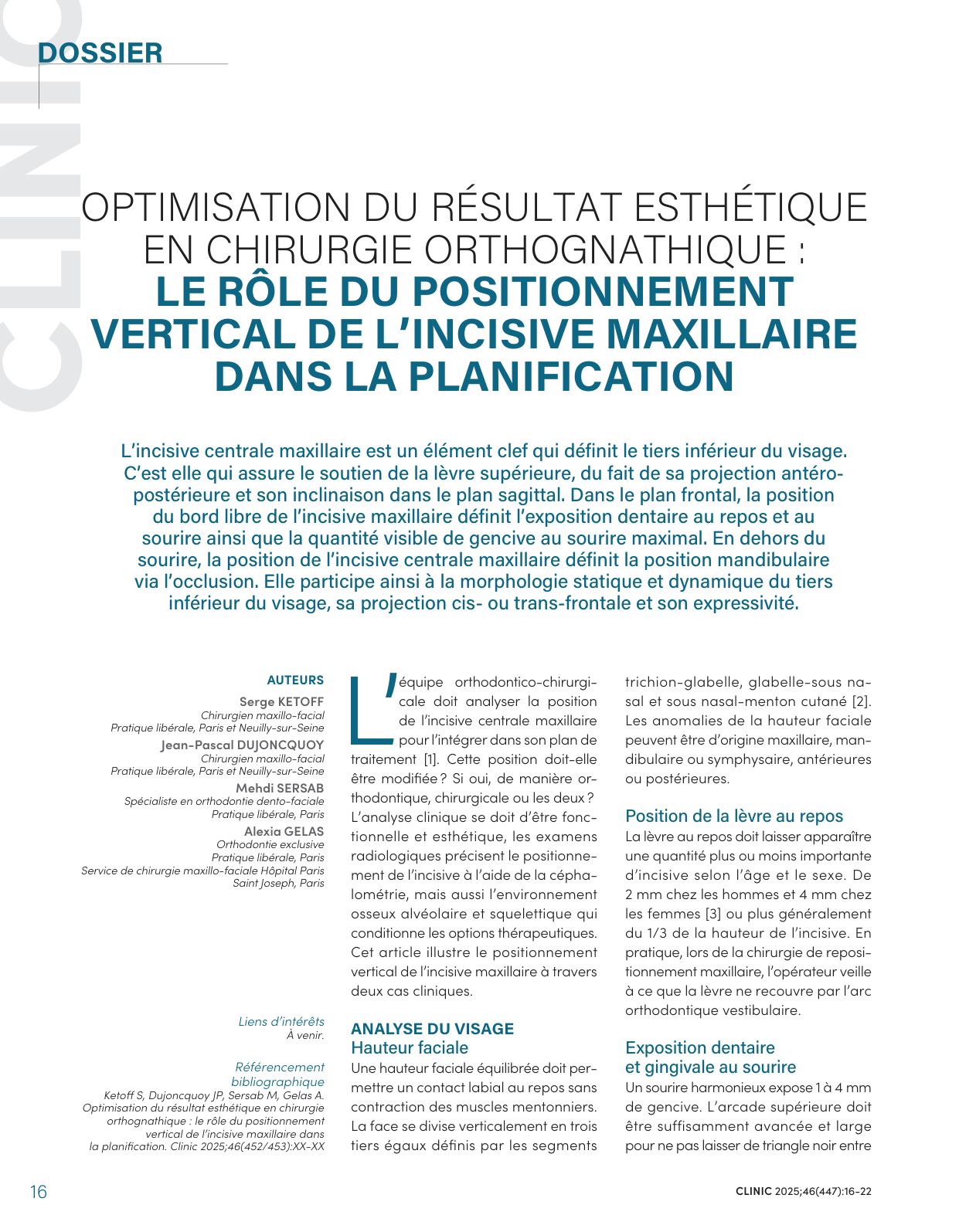
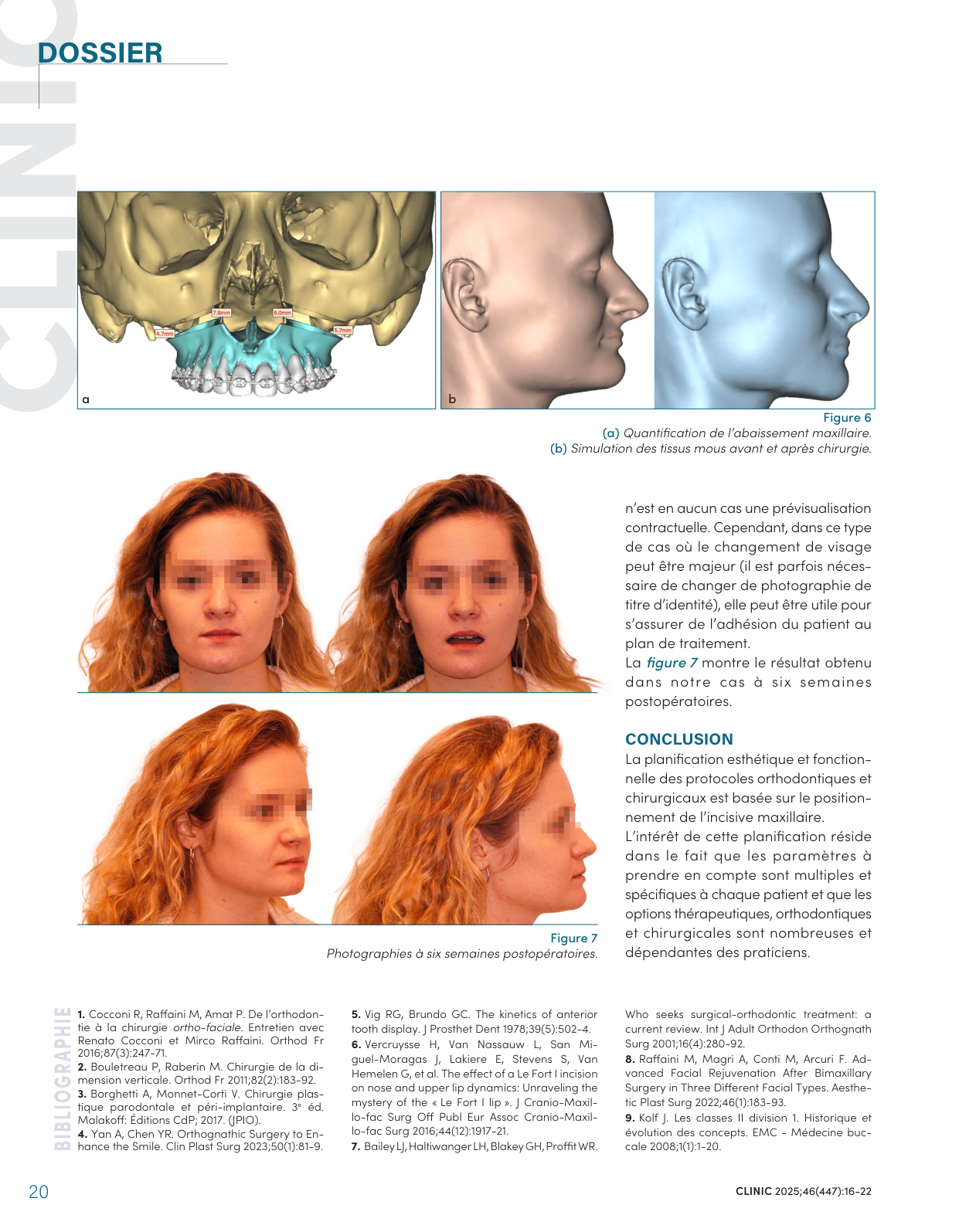
The patient presents with a short, square-looking face, no incisor display with the mouth slightly open, marked nasolabial folds and a closed nasolabial angle. The objective is the opposite: to increase facial height and achieve incisor display at rest. The maxillary downgrafting is calculated by adding the preoperative incisor-to-lip distance (3 mm) and the desired display (4 mm), with overcorrection — 8 mm in this case. Lengthening genioplasty adjusts the height of the lower third without increasing the maxillary downward movement. 3D surgical planning above all quantifies the gap to be grafted at the osteotomy site to ensure bone healing.
Key Takeaways
The aesthetic and functional planning of orthodontic-surgical protocols is based on the positioning of the maxillary incisor. The parameters to consider are numerous and specific to each patient; digital soft tissue simulation, useful for patient adherence to the treatment plan, must be presented with caution as it in no way constitutes a contractual preview.
Reference: Ketoff S, Dujoncquoy JP, Sersab M, Gelas A. Optimisation du résultat esthétique en chirurgie orthognathique : le rôle du positionnement vertical de l'incisive maxillaire dans la planification [Optimizing the aesthetic outcome in orthognathic surgery: the role of the vertical position of the maxillary incisor in planning]. Clinic 2025;46(452/453).