Maxillary Endognathia: Decision Criteria and Treatment Strategies
Yoann-Luc Vu Van Tuan · Jean-Pascal Dujoncquoy · Serge Ketoff
CLINIC No. 452/453 · July–August 2025
Maxillary endognathia is defined as a reduction in maxillary width, often affecting respiratory function, occlusion and facial aesthetics. Common in orthodontics, particularly in young adults, it is frequently associated with mouth breathing, a narrow palate and underdeveloped nasal cavities. Restoring an adequate transverse dimension is key to treatment stability: good occlusion and an ideal functional pattern for tongue position, essential for physiological swallowing and breathing.
A Rigorous Clinical and Radiological Diagnosis
The examination focuses on occlusion but must include a facial and functional analysis: palatal shape (high-arched if the tongue has remained in a low position), narrow nasal cavities in mouth breathers, arch overlap. The transverse deficiency is measured between the mesiopalatal cusps of the maxillary first molars and the central fossae of the mandibular molars, taking into account dental compensations that may mask it. Beyond a 3 to 4 mm deficiency, orthopedic or surgical treatment should be considered; functional rehabilitation (physiotherapy, speech therapy) must always accompany this type of treatment.
Orthopedic Expansion, Surgically Assisted Expansion or MARPE?
In children, orthopedic rapid palatal expansion widens the still-flexible midpalatal suture: anchorage on the primary molars, one activation per day, up to 10 mm of transverse gain, with an associated increase in nasal cavity volume that improves respiratory function.
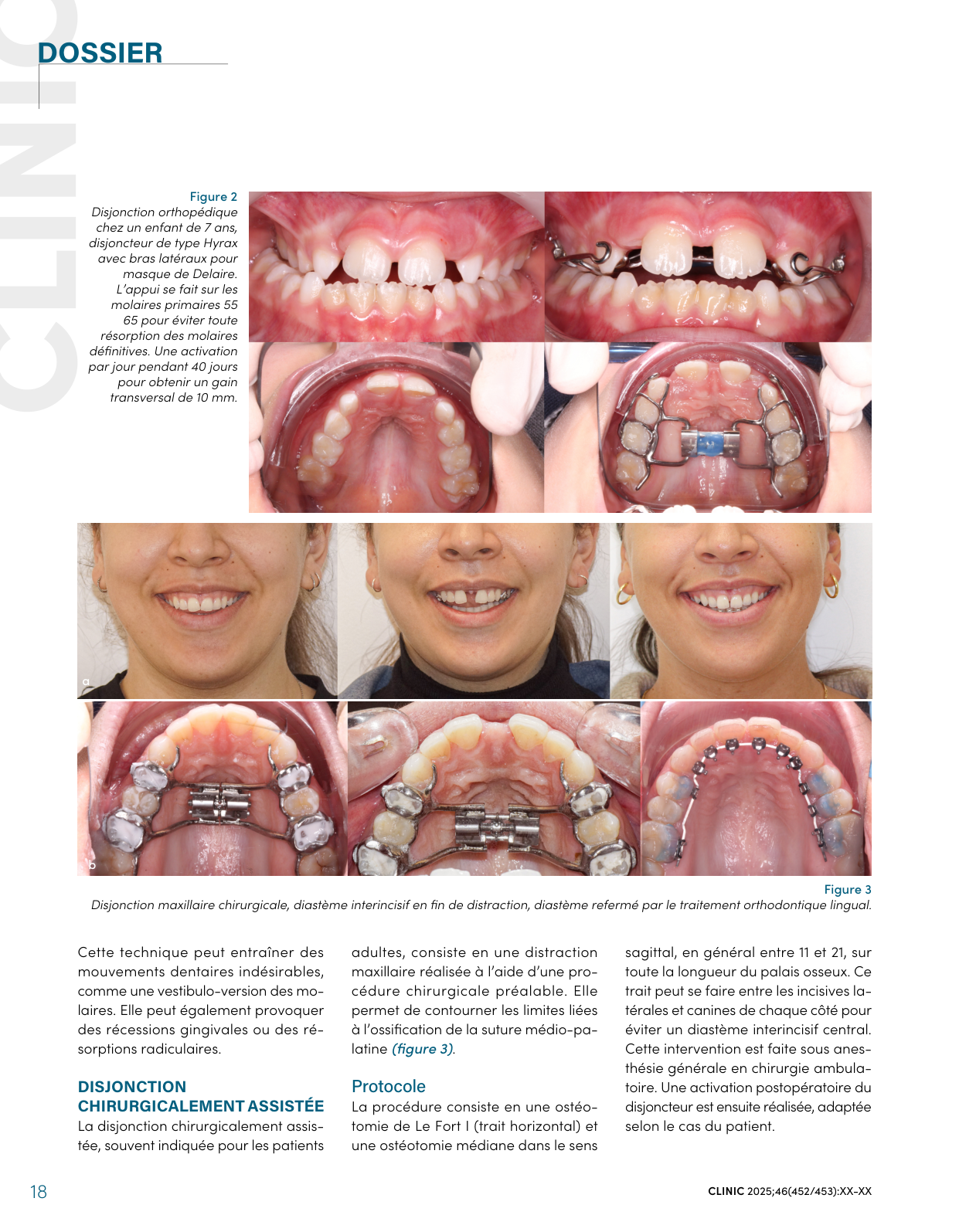
In adults, the suture is often ossified: surgically assisted rapid palatal expansion (SARPE) combines a Le Fort I osteotomy with a midline palatal osteotomy, performed as outpatient surgery. After a latency period of 7 to 10 days, the expander is activated by 0.25 to 0.5 mm per day, then left in place for 3 to 6 months to stabilize the result. Surgery is also an opportunity for associated procedures: widening of the nasal cavities, wisdom tooth removal, bone grafting under a thin periodontium, or alveolar corticotomies.
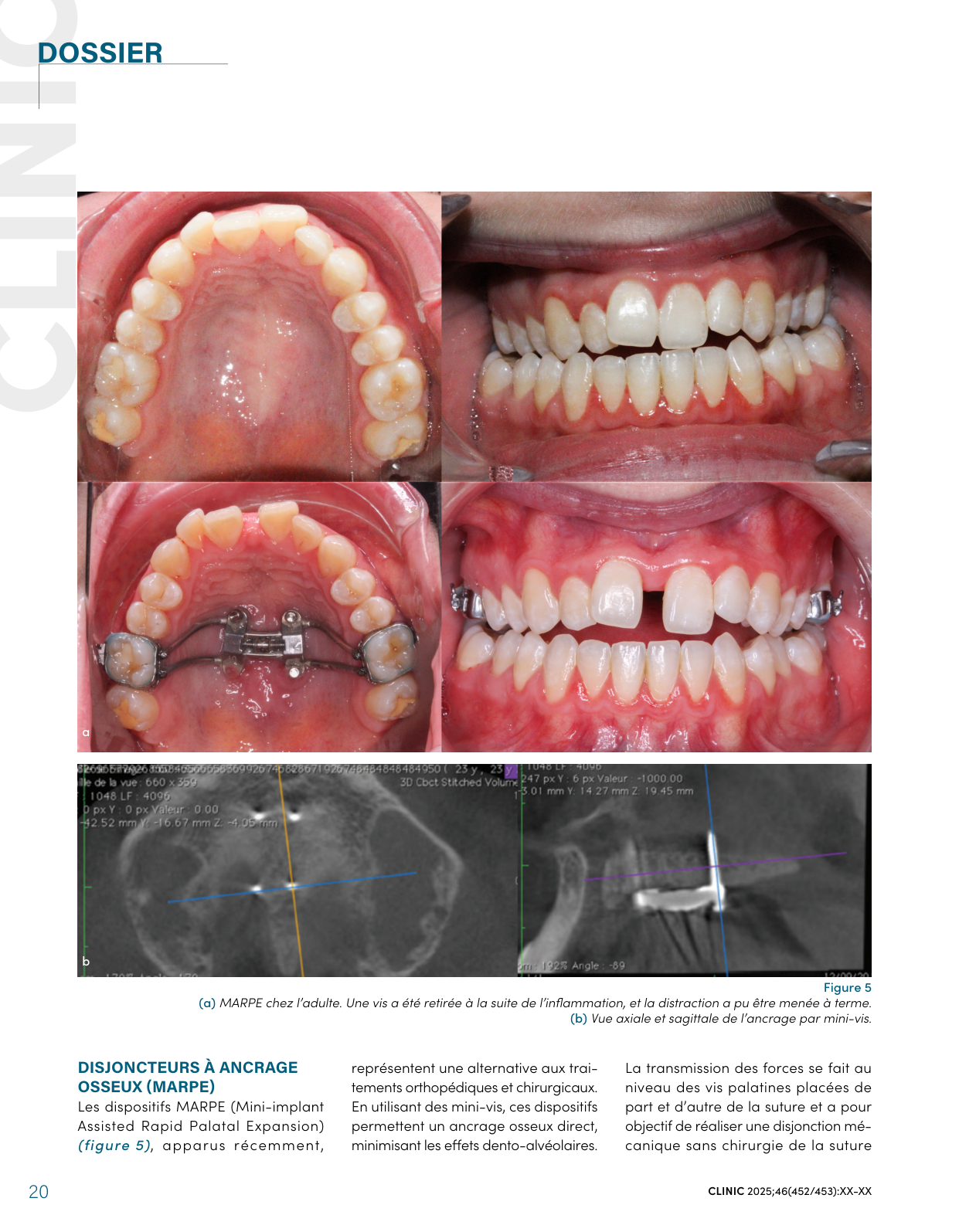
More recently, MARPE devices (Mini-implant Assisted Rapid Palatal Expansion) transmit force directly to the bone via palatal mini-screws, under local anesthesia, and can avoid surgery in selected cases. The reported success rate is approximately 85 %, highly dependent on patient selection and the status of the midpalatal suture.
How to Choose? Age, Sutural Maturation, Periodontium
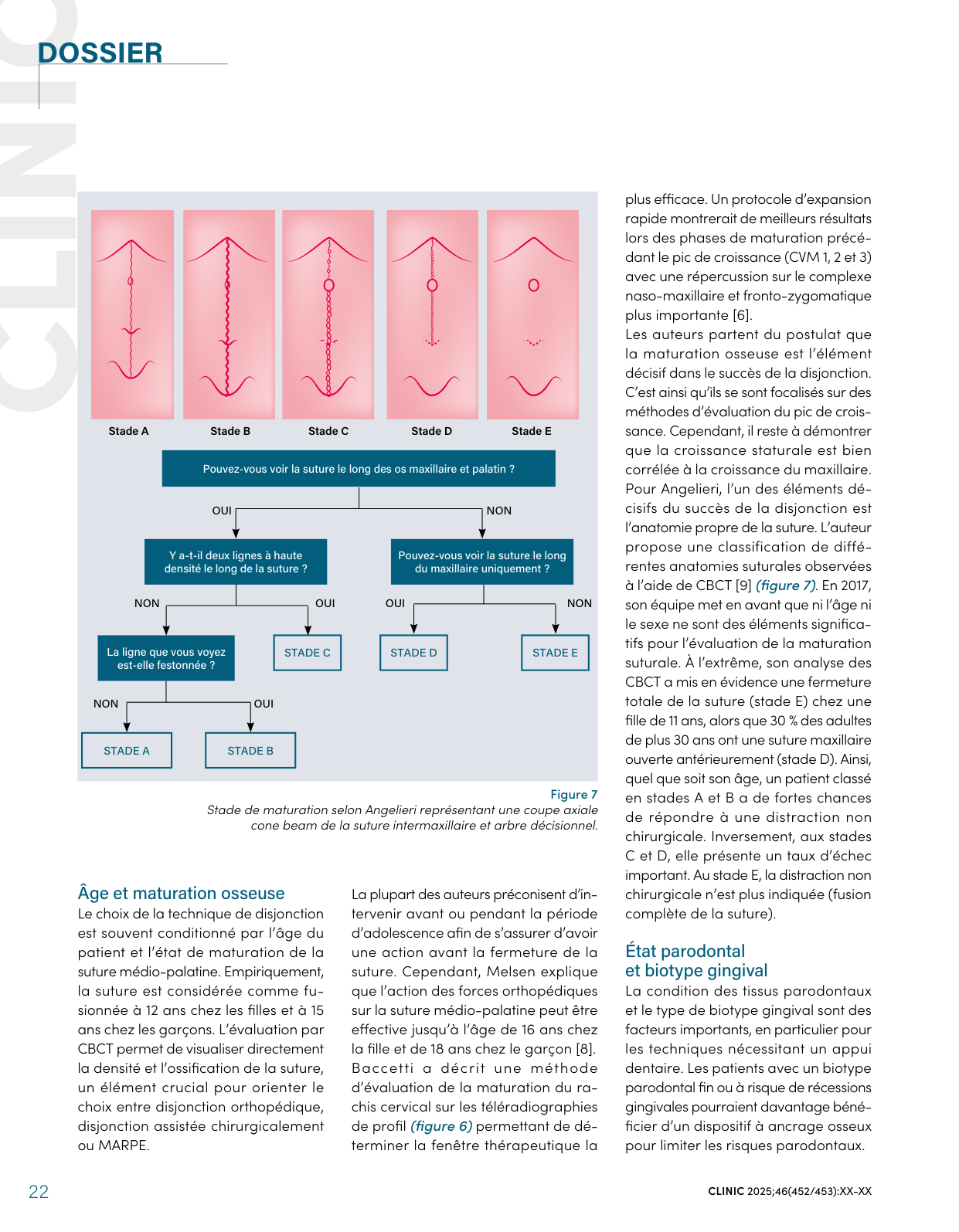
Chronological age is not sufficient: cervical vertebral maturation (Baccetti method) and, above all, the anatomy of the suture observed on CBCT (Angelieri classification, stages A to E) guide the decision. An 11-year-old girl may present a fully fused suture, while 30 % of adults over 30 retain an anteriorly open suture. At stages A and B, non-surgical expansion has a high chance of success; at stage E, it is no longer indicated. Periodontal status also matters: a thin gingival biotype favors a bone-borne device to limit recessions.
A Comprehensive Approach
Expansion techniques have evolved with minimally invasive surgery (piezosurgery, reduced surgical approaches), bone-borne devices and CBCT imaging. The goal remains stability of the expansion and of the occlusion — without neglecting functional management (tongue and breathing rehabilitation) and ENT screening for airway obstruction.
Reference: Vu Van Tuan YL, Dujoncquoy JP, Ketoff S. Endognathie maxillaire : critères décisionnels et stratégies de traitement [Maxillary endognathia: decision criteria and treatment strategies]. Clinic 2025;46(452/453).